The Gold Standard in Safety: Integrating Advanced Anatomy and Emergency Protocols in Facial Volumization
The evolution of medical aesthetics has shifted the focus from simple volumization to high-precision structural rejuvenation. However, as injection depth and product complexity increase, so does the risk of vascular compromise. For the aesthetic physician, clinical success is no longer defined solely by the aesthetic result, but by the systematic integration of vascular safety protocols facial fillers practitioners must master. This guide provides an in-depth analysis of instrument selection, anatomical danger zones, and the physiological management of vascular events.
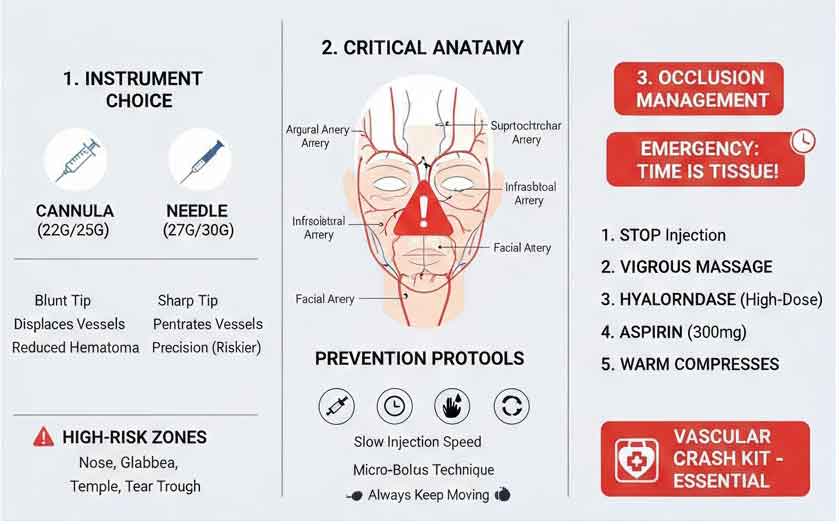
1. Instrument Engineering: The Clinical Rationale for Cannulas
The debate between needle and cannula is not merely a matter of comfort but of physics and safety. The blunt tip of a micro-cannula (typically ≥25G) is designed to resist the penetration of arterial walls, whereas the beveled edge of a needle facilitates effortless entry into any vessel in its path.
Table 1: Technical Selection and Gauges by Anatomical Zone
| Anatomical Zone | Instrument Recommended | Suggested Gauge | Clinical Justification |
| Temple (Subfascial/Interfascial) | Cannula | 22G – 25G | Protects the superficial temporal artery and reduces risk of venous emboli. |
| Tear Trough | Cannula | 25G | Essential for the thin periorbital skin to prevent hematomas and infraorbital artery injury. |
| Lip Body & Border | Needle | 30G | Required for precise definition and managing high-viscosity products in small volumes. |
| Midface & Malar | Cannula | 22G | Large-bore cannulas allow for even distribution across the sub-SMAS planes with minimal trauma. |
| Nasal Dorsum (Liquid Rhinoplasty) | Cannula | 25G | Highest Risk Zone. Cannulas reduce the risk of dorsal nasal artery occlusion. |
| Jawline & Mandibular Angle | Cannula | 22G | Ideal for long, linear retrograde threads along the mandibular border. |
2. Anatomical “Red Zones”: Identifying High-Risk Vasculature
Understanding 3D facial anatomy is the primary defense against catastrophic complications such as skin necrosis or iatrogenic blindness. Clinicians must recognize that vascular patterns often deviate from textbook descriptions.
The Danger Zone Hierarchy
- The Glabella and Forehead: The supratrochlear and supraorbital arteries are terminal branches of the ophthalmic artery. Intra-arterial injection here can lead to retrograde flow into the retinal artery, causing irreversible blindness within minutes.
- The Nasolabial Fold (NLF): The angular artery is superficial in this region. Many practitioners erroneously assume that deep injections are safe, but the artery can be found at varying depths.
- The Pyriform Aperture: Deep injections for NLF correction are close to the angular artery’s origin. Use of a cannula is strongly advised when performing deep bolus injections.
- The Alar Groove: This is a watershed area with limited collateral circulation. Even minor compression or small emboli can lead to rapid necrosis of the nasal ala.
3. The Science of Prevention: Advanced Injection Techniques
To mitigate risk, the practitioner must adopt a “Safety-First” mindset, moving beyond the basic aspiration test.
The Limitation of Aspiration
Research indicates that aspiration has a high false-negative rate. The vacuum created can collapse a small vessel wall against the needle tip, preventing blood return even if the needle is intravascular.
- Clinical Pearl: Aspiration must be performed for at least 10 seconds, but should never be the sole indicator of safety.
Rheology and Pressure
The “Injection Pressure” is a critical variable. High extrusion force, often needed for high-G’ (viscosity) fillers, increases the speed of an embolus if a vessel is breached.
- Low-Flow Technique: Always inject slowly. Use the minimum pressure required to move the product. This allows for early detection of pain or blanching.
- Micro-bolus and Fanning: Avoid large boluses in high-risk areas. Small, multiple passes (0.05cc to 0.1cc) reduce the risk of extrinsic vascular compression.
4. Emergency Management: The “Time is Tissue” Protocol
A vascular occlusion (VO) is a medical emergency. The therapeutic window to prevent permanent scarring or necrosis is narrow. Every clinic must have a “Vascular Crash Kit” ready for immediate deployment.
Recognizing the Signs
- Stage 1: Immediate blanching or “ashy” skin tone.
- Stage 2: Disproportionate, crescendo pain (though some VOs are painless).
- Stage 3: Livedo Reticularis (a bluish, net-like pattern indicating venous congestion or arterial blockage).
- Stage 4: Pustule formation and eventual tissue breakdown.
Table 2: The High-Dose Pulsed Hyaluronidase Protocol
| Step | Intervention | Technical Detail |
| Step 1 | Immediate Cessation | Stop the procedure. Do not remove the cannula if it can be used for irrigation. |
| Step 2 | Hyaluronidase (H-D) | Inject 500–1500 units of Hyaluronidase into the affected area and along the vessel path. |
| Step 3 | Massage | Firm, vigorous massage to promote enzymatic contact and break up the filler. |
| Step 4 | Aspirin Therapy | 300mg oral aspirin to prevent further platelet aggregation and clot propagation. |
| Step 5 | Heat & Vasodilation | Apply warm compresses for 15 minutes every hour to encourage collateral flow. |
5. Conclusion: Ethics in Aesthetic Medicine
Vascular safety is not an elective skill; it is the foundation of ethical aesthetic practice. By transitioning to large-bore cannulas in high-risk zones, mastering the anatomy of facial danger zones, and maintaining a rigorous emergency protocol, clinicians can minimize the incidence of adverse events.
The ultimate goal of the aesthetic physician is to enhance beauty without compromising the biological integrity of the patient.
Sources and Clinical References (Academic URLs)
- Journal of Clinical and Aesthetic Dermatology (JCAD): Vascular Complications of Dermal Fillers: Prevention and Management
- Aesthetic Surgery Journal (ASJ): Consensus on Managing Vascular Occlusions and Hyaluronidase Protocols
- Plastic and Reconstructive Surgery: The Anatomy of Facial Danger Zones for Fillers
- Dermatologic Surgery Journal: Aspiration Before Tissue Filler – An Exercise in Futility?