
Intralipotherapy, or the non-surgical dissolution of localized fat deposits, has become a cornerstone of aesthetic medicine. Among the available solutions, Aqualyx® has established itself as one of the most widely used and studied adipocytolytic agents in Europe. However, its efficacy and safety are contingent on a thorough understanding of its mechanism of action, a strict preparation protocol, and a precise infiltration technique.
This article is an advanced clinical guide, intended exclusively for medical professionals, that breaks down the complete Aqualyx protocol—from dilution and preparation to zone-differentiated infiltration techniques (submental vs. corporate) and the management of complications.
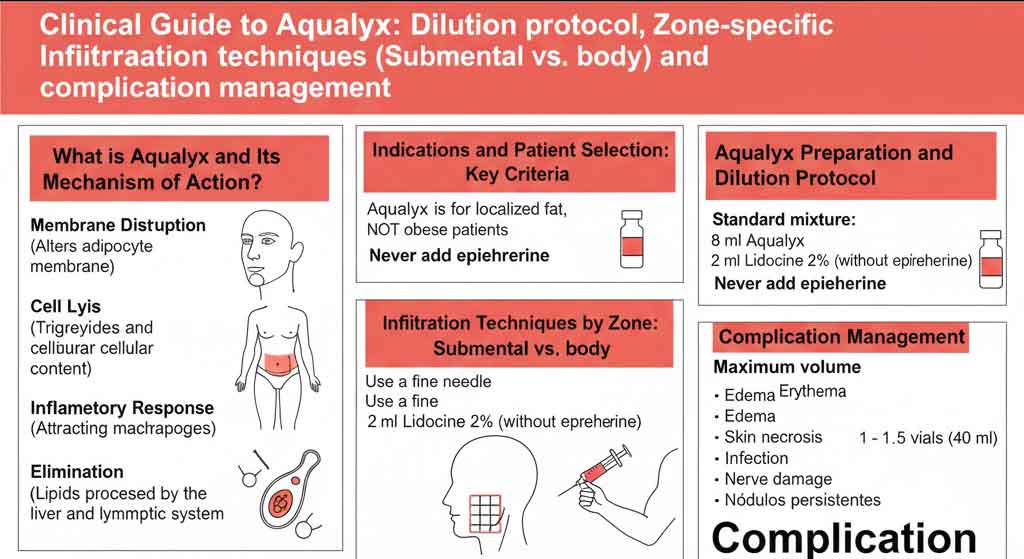
What is Aqualyx and its Adipocytolytic Mechanism of Action?
Aqualyx is a micro-gelatinous, biocompatible, and biodegradable solution that contains a polymer of 3,6-dihydroxy-10-ethyl-hexadecanoyl-choline and sodium deoxycholate. Although often associated with phosphatidylcholine, the primary active agent is sodium deoxycholate.
Sodium deoxycholate, a secondary bile salt, acts as a biological “detergent.” Its mechanism of action is adipocytolysis:
- Membrane Disruption: The deoxycholate alters the surface tension of the adipocyte (fat cell) membrane.
- Cell Lysis: It causes lysis and vacuolization of the cell membrane, releasing triglycerides and cellular content into the interstitial space.
- Inflammatory Response: This triggers a localized inflammatory response, attracting macrophages to phagocytose the released lipids and cellular debris.
- Elimination: The lipids are processed by the liver and eliminated through the lymphatic system and the usual metabolic pathway.
It is crucial to understand that Aqualyx causes permanent cell necrosis of the treated adipocyte. It is not a treatment for weight loss, but for facial and body contouring by eliminating resistant localized fat.
Indications and Patient Selection: Key Criteria
Treatment success begins with impeccable patient selection. The ideal candidate for Aqualyx is not a patient who is overweight or obese (BMI > 30), but rather one with localized fat deposits (localized adiposity) that persist despite diet and exercise.
Common Indications:
- Facial: Submental fat (double chin).
- Body: Abdomen (upper and lower), flanks (“love handles”), “saddlebags” (trochanters), inner thighs, knees, “buffalo hump,” and pseudogynecomastia.
Absolute Contraindications:
- Pregnancy and lactation.
- Significant liver or kidney disease (due to the lipid metabolization pathway).
- Coagulation disorders or use of anticoagulants (increases risk of hematoma).
- Active autoimmune diseases or uncontrolled diabetes.
- Active infection at the injection site.
- Known allergy to any of the components.
- Severe skin laxity (fat removal can worsen laxity).
Aqualyx Preparation and Dilution Protocol
One of the most frequent questions is the dilution protocol for Aqualyx. It is essential to follow guidelines to ensure patient safety and comfort.
Materials Needed:
- Vials of Aqualyx (usually 8 ml).
- Lidocaine 2% (without epinephrine).
- Sterile syringes (10 ml or 20 ml).
- Drawing-up needles (18G or 20G).
- Intralipotherapy cannulas (e.g., 24G 70mm or 100mm for body) or fine needles (e.g., 27G or 30G for chin).
- Antiseptic solution (chlorhexidine).
The “Dilution” Protocol (Addition of Anesthetic)
Aqualyx is formulated for use, but infiltration into adipose tissue can be painful. Therefore, the standard protocol involves the addition of an anesthetic.
Professional Warning: Never add epinephrine (adrenaline) to the mixture. Epinephrine induces vasoconstriction, which, when combined with a cytolytic agent, can significantly increase the risk of skin necrosis.
Standard Mixture Ratio:
- 8 ml of Aqualyx
- 2 ml of Lidocaine 2% (without epinephrine)
This mixture provides a total volume of 10 ml per vial, which facilitates dose calculation per area and significantly improves the patient’s tolerance of the procedure. A rigorous aseptic technique must be performed throughout the mixing and preparation process.
Infiltration Techniques by Zone: Submental vs. Body
The infiltration technique is not universal; it must be anatomically adapted to the treatment area, considering the depth of the fat and the proximity of vital structures.
1. Submental Area (Double Chin): Precision and Safety
Treating the double chin requires absolute precision due to the proximity of the marginal mandibular nerve and the facial artery.
- Marking: Mark the treatment area (pre-platysmal fat). Ask the patient to smile to identify the border of the platysma muscle and the course of the marginal mandibular nerve (usually 1-2 cm below the mandibular border). Always stay inferior and posterior to this “exclusion zone.”
- Technique: The use of a fine needle (27G or 30G) for micro-depot injections is preferred.
- Depth: The needle must penetrate the dermis and be placed in the center of the pre-platysmal adipose tissue (approx. 6-10 mm depth). A too-superficial (dermal) injection can cause skin necrosis.
- Dosage: Inject 0.1 ml – 0.2 ml per injection point.
- Spacing: Points should be 1 cm – 1.5 cm apart.
- Maximum Volume: Do not exceed 1 to 1.5 vials (8-12 ml of product) per session in this area.
- Sessions: Generally 2-4 sessions, spaced 4-6 weeks apart.
2. Body Areas (Abdomen, Flanks, Saddlebags)
Body treatment allows for the use of larger volumes and a different, more efficient technique for large areas.
- Marking: Demarcate the area to be treated in 10×10 cm grids.
- Technique: Intralipotherapy with a cannula (e.g., 24G, 70mm or 100mm) is the technique of choice. It is performed through 1 or 2 entry points per grid.
- Method: A fanning or linear threading (retrograde tunnels) technique is used. The solution is deposited uniformly as the cannula is withdrawn.
- Depth: The cannula must be placed in the deep subcutaneous fat, just above the muscle fascia. Depth varies (10-15 mm) depending on the area and patient. Avoid intramuscular injections.
- Dosage: 0.3 ml – 0.5 ml per retrograde tunnel.
- Spacing: Tunnels should be 1.5 cm – 2 cm apart.
- Maximum Volume: Generally, one 8 ml vial (or 10 ml of mixture) is administered per 10×10 cm grid. Do not exceed 40 ml (5 vials) per session on the body.
- Sessions: Generally 3-8 sessions, spaced 3-4 weeks apart.
Management of Complications and Post-Treatment Care
The practitioner must know how to differentiate between expected sequelae (unavoidable consequences of inflammation) and real complications (adverse events).
Expected Sequelae (Normal and Self-Limiting)
- Edema (Swelling): This is the most common sequela and can be significant, especially in the double chin (the “pelican effect”). It is a sign that the product is working (inflammatory response). It lasts 3 to 7 days.
- Erythema and Warmth: Signs of inflammation.
- Pain and Tenderness: Manageable with simple analgesics (paracetamol). It is recommended to avoid NSAIDs (like ibuprofen) for the first 48 hours, as they may interfere with the desired inflammatory response.
- Bruising: Common, especially if a needle is used.
- Temporary Nodules: Small areas of induration that are part of the inflammatory process.
Real Complications (Rare but Serious)
- Infection/Abscess: Result of poor aseptic technique. Requires drainage and antibiotic therapy.
- Skin Necrosis: The most feared complication. Occurs if the product is injected too superficially (intradermally). It manifests as a violaceous, pale, and painful plaque that can ulcerate. Requires immediate specialized management.
- Nerve Damage (Paresis): Specific to the double chin (injury to the marginal mandibular nerve). It is usually a temporary neurapraxia (paresis) that recovers in weeks, but it is alarming for the patient.
- Persistent Nodules/Fibrosis: Nodules that do not resolve after 4-6 weeks. May require massage, therapeutic ultrasound, or, in rare cases, corticosteroid infiltration.
- Contour Irregularities: Result of an uneven infiltration technique.
Post-Treatment Protocol for the Patient
Instructing the patient is vital for managing their expectations and optimizing results.
- Compression: Using a compression garment (body) or a chin strap (facial) for 24-72 hours can help reduce edema and improve comfort.
- Local Cooling: Apply intermittent cold (never directly on the skin) during the first 24 hours.
- Avoid Heat: Do not apply heat (saunas, hot baths, sun) to the area for 48-72 hours.
- Hydration: Drink plenty of water to help the lymphatic system clear the lipids.
- Exercise: Avoid high-intensity exercise for 3-5 days.
- Massage: Some protocols recommend a gentle lymphatic drainage massage 5-7 days after treatment to help reduce edema and prevent irregularities.
Conclusion: Integrating Aqualyx into Your Clinical Practice
Aqualyx is a potent and effective tool for non-surgical lipolysis, but it demands respect for anatomy and technique. Unlike hyaluronic acid fillers, errors in injection depth can have serious consequences, such as skin necrosis.
Success lies in three pillars: rigorous patient selection, an infiltration technique adapted to the zone (correct depth and dosage), and transparent management of expectations and sequelae with the patient. By mastering this protocol, medical professionals can offer safe and consistent facial and body contouring results.
Reference Sources
- Marllor Biomedical (Manufacturer): Product information and scientific basis. (Reference link: https://www.aqualyx.it/)
- Study on Sodium Deoxycholate (NCBI): Deoxycholic Acid in the Submental Area – A fundamental study on the mechanism and safety of the active ingredient in the submental area. (Reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4443900/)